|
|
|
| Wooden Foreign Body In Symphysis Region Of Mandible: A Rare Case Report |
Anil Kumar 1 , Monika Parmar 2 , Abhishek Soni 3 , Mohinder Chandel 4
1 Senior Lecturer, Dept. of Oral & Maxillofacial Surgery - H.P. Government Dental College & Hospital, Shimla
2 Senior Lecturer, Department of Oral and Maxillofacial Surgery - H.P. Government Dental College & Hospital, Shimla
3 Senior Lecturer, Department of Oral and Maxillofacial Surgery - H.P. Government Dental College & Hospital, Shimla
4 Junior Resident, Department of Oral and Maxillofacial Surgery - H.P. Government Dental College & Hospital, Shimla
|
| Address For Correspondence |
Dr. Anil Kumar, Senior Lecturer
Department of Oral and Maxillofacial Surgery,
H.P. Government Dental College & Hospital, Shimla.
Phone : 919625309445
Email ID: sushma_chugh@yahoo.co.in |
| Abstract |
| A wooden piece was retrieved from symphysis region of the mandible after one year of injury. The case presented here underlines the importance of thorough history, proper investigations and considerations of presence of foreign body in cases of long standing infections. |
|
| Keywords |
| Symphysis, foreign Body, Hyperdense, chin, CT scan |
|
| Full Text |
Introduction
Head and neck infections occur frequently, common causes include odontogenic and cutaneous lesions[1]. Foreign bodies are sometimes encountered in the face[2], occasionally foreign bodies may be retained for some time causing persistent and distressing symptoms[3], Most cases occur in infants and children and are usually accompanied by poor history and difficulty in clinical examination, which may be a problem to establish an accurate diagnosis[4].
Case Report
A 14 year old male patient reported to the Department of Oral & Maxillofacial surgery with chief complaint of non healing wound in chin area since last one year.
According to the parents the patient was apparently well one year ago when he fell from a tree and sustained injury in chin region. Patient was taken to a nearby community health centre where dressing of wound was done after suturing of laceration and antibiotics were prescribed. But after a week pus started oozing from the wound. The wound was re-explored and again dressing was done. This time intravenous antibiotics were prescribed. The wound healed but after 3 months again there was a pus discharge. This time radiograph was taken. Patient was diagnosed with osteomyelitis and was prescribed antibiotics for 15 days. The wound healed but after about 2 months again pus discharging sinus appeared. Patient was referred to District Hospital but patient preferred to come to Department of Oral & Maxillofacial Surgery at Himachal Pradesh Government Dental College Shimla.
Patient was not a known case of Diabetes mellitus/Hypertension/Asthma/Epileps.
On extra oral examination, a 2x2 c.m. single sinus in the submental region with granulation tissue at the opening of sinus and discharging pus was present. Sinus was tender, mobile and with thick walls.
On intraoral examination no abnormality was detected.
Based on examination OPG and C.T. scan was taken.
In OPG nothing abnormal was detected but C.T. scan showed increase in soft tissue in chin region anteriorly. There was an evidence of hyperdense irregular 9x7m.m. foreign body focus with a density of 156 H.U. (Fig 1 - a, b, c), however there was no evidence of any erosive destruction or fracture of mandible.
 | Fig 1a: Sagittal View
 |
 | Fig 1b: Axial View
|
 | Fig 1c: Coronal View
|
Based on C.T. scan observations, surgical exploration of soft tissue with removal of foreign body was planned under local anesthesia.
CT scan showing hyperdense area in anterior chin region
Operative Procedure
Surgical exploration was done with mandibular vestibular incision in the anterior region under local anesthesia, layer by layer blunt dissection was done, wooden piece was removed and curettage was done. Communication between intra and extraoral wound was explored and epithelial lining was removed. Layer by layer suturing intraorally was done with vicryl 3-0 and mucosa with 4-0 silk. Medications were prescribed and regular follow up was done. (Fig 2, 3)
 | Fig 2: Surgical Exposure
|
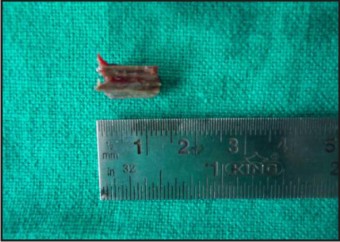 | Fig 3: Foreign Wooden Piece
|
Discussion
A few reports on wooden foreign bodies in head or neck have appeared in international literature, most involving pieces of wood or branches, fish bones, incisor fragments, fragments of smoking pipes, disposable broken bur[5],[3]. Tissue reactions from foreign bodies are commonly encountered in oral cavity[6]. Retained foreign bodies are capable of causing inflammation, abscess formation as well as chronic pathologies including granulomatous tissue reaction, fistula formation and osteomyelitis[7]. Wood and bamboo, with their porous consistency and organic nature, provide a good medium for microbial agents[8]. Foreign bodies made from metal, plastic, glass are easily detected with an ordinary x-ray. However wooden foreign bodies are difficult to detect in ordinary x-ray, so their diagnosis is often missed or delayed [9],[10]. C.T. is considered the gold standard for detection of foreign bodies[11]. Magnetic resonance imaging (MRI) may be more sensitive when the wooden foreign body is embedded in fat (i.e. orbital fat). If C.T. scans do not reveal a suspected wooden fragment, MRI should be carried out[10]. The correct diagnosis of a retained wooden foreign body is often difficult because it may follow relatively minor trauma, and may not be identified clinically[10].
Penetrating foreign bodies may present diagnostic challenge to the trauma surgeon and foreign body should always be considered in the differential diagnosis of a case presenting with a draining sinus apart from osteomyelitis and fracture.
References
1. M. Cameron, B. Phillips: SnookeredN82; Facial infections secondary to occult foreign body: Int.J.Oral Maxillofac Surg. 2006; 35: 373-375.
2. Da Silva EJ, Deng Y, Tumushime Buturo CG: An unusual foreign body in the tongue: Br J Oral Maxillofac Surg. 2000; 38: 241-242.
3. Robinson PD, Rajayogeswaran R, Orrr: Unlikely foreign bodies in unusual facial sites: Br J Oral Maxillofac Surg 1997; 35: 36-39.
4. Andre Croli Rocha, Daniel Galera Bernabe, et al: Foreign body in the hard palate of children and risk of misdiagnosis: report of three cases: J.Oral Maxillofac Surg. 2009; 67: 899-902.
5. Hiroyuki Wakisaka, Hirotoka Takahashi, et al: A case of wooden foreign body penetrating the oral cavity and reaching the posterior neck: J.Injury. 2010; 41: 92-96.
6. Ehab Shehata, Kholoud Moussa, et al: A foreign body in the floor of the mouth: j.sdentj. 2010; 22: 141-143.
7. Amin M. Nasr, Barrett G. Haik, et al: Penetrating orbital injury with organic foreign bodies: j. ophthal. 1999; 106: 523-532.
8. K.G.H. van der Wal, R.J. Boukes: Intraorbital bamboo foreign body in a chronic stage: case report: Int.J.Oral Maxillofac Surg. 2000; 29: 428-429.
9. Hideki Imokawa, Takasi Tazawa, et al: Penetrating neck injuries involving foreign bodies: Int.J.Orl & HNS. 2003; 30: 145-147.
10. M. Krimmel, C.P. Cornelius, et al: Wooden foreign bodies in facial injuries: a radiological pitfall: Int.J.Oral Maxillofac Surg. 2001; 30: 445-447.
11. Pierre-John Holmes, Jason R. Miller, et al: Intraoperative imaging techniques: A guide to retrieval of foreign bodies: Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100: 614-618. |
|
|
|
|
|
|